
Author: Matthew Wells, DO
Description
Fibrous dysplasia is a benign (non-cancerous) bone condition in which normal bone is replaced by abnormal fibrous (scar-like) tissue mixed with immature bone. This can make the affected bone weaker than normal, which may lead to pain, deformity, or fractures over time.
Fibrous dysplasia may affect only one bone (called monostotic fibrous dysplasia) or multiple bones (called polyostotic fibrous dysplasia). In rare cases, fibrous dysplasia can occur along with skin pigment changes (such as café-au-lait spots) and hormone-related problems, a condition known as McCune-Albright syndrome. Fibrous dysplasia is most often diagnosed in children, teenagers, and young adults, although it can be found at any age. It is considered a developmental bone disorder caused by a genetic change that happens early in development. This genetic change is not inherited, which means fibrous dysplasia is not passed from parents to children or from patients to their children.
Symptoms
The timing of the genetic change during development often affects how much of the body is involved and how severe the condition may be. In general, the earlier this change happens, the more bones may be affected and the more noticeable the symptoms can be.
Many people with fibrous dysplasia have mild symptoms or no symptoms at all. When symptoms do occur, they often include a dull, aching pain in the affected bone that may get worse with activity, exercise, or sports. As the abnormal fibrous tissue grows and weakens the bone, some patients may develop a bone deformity. For example, the thigh bone (femur) may slowly bend over time, creating what doctors sometimes call a “shepherd’s crook” deformity (Figure 1).
In more severe cases, the bone may become weak enough to break with little or no injury. This is called a pathologic fracture.
Examination
During the physical exam, your doctor may notice tenderness (pain when pressing) over the affected bone, a visible bone deformity, or a limp if the legs are involved. If the bone has become weak enough to break (pathologic fracture), there may also be swelling, bruising, or more severe pain in that area. In patients with McCune-Albright syndrome, the doctor may also notice flat, light-brown skin patches, called café-au-lait spots, on different areas of the body.
Tests
Blood tests are usually normal in patients with fibrous dysplasia. X-rays are usually the first and most important imaging test used to diagnose fibrous dysplasia. In many cases, X-rays provide enough information to make the diagnosis. A CT scan or MRI may be ordered if your doctor needs a more detailed look at the bone, wants to better understand the size and location of the lesion, or if there is concern for a fracture or bone deformity. In some cases, a bone scan may be recommended to see whether more than one bone is affected. A biopsy (taking a small sample of bone tissue) is usually not needed, unless the imaging findings look unusual or there is concern for another possible diagnosis.
Images
On X-rays, fibrous dysplasia often appears as an area of cloudy or hazy bone, sometimes described by doctors as having a “ground glass” appearance (Figure 1). Over time, if the condition weakens the bone, it can sometimes cause the bone to slowly bend or change shape. For example, fibrous dysplasia in the thigh bone (femur) may lead to a curved deformity known as a “shepherd’s crook” deformity (Figure 2).

Figure 1. Anterior-posterior (AP) X-ray of a humerus (upper arm) demonstrating the classic “ground glass” appearance (red arrow) of fibrous dysplasia.
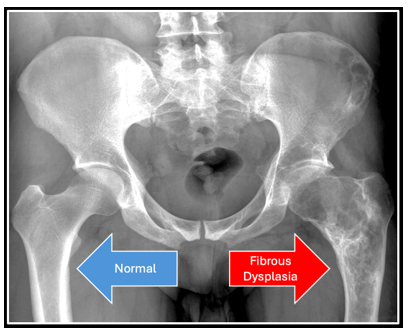
Figure 2. Anterior-posterior (AP) X-ray of the pelvis demonstrating the “shepherd’s crook” bowing deformity caused by fibrous dysplasia weakening the bone over time.
Prognosis
Fibrous dysplasia is not cancer, which means it does not spread to other parts of the body. However, it can affect one bone or multiple bones and may cause ongoing pain, bone deformity, or an increased risk of fractures over time. In most patients, the growth of fibrous dysplasia slows down after the skeleton finishes growing, usually after puberty. Many patients with monostotic fibrous dysplasia (only one bone affected) have a mild course and do well with observation and regular follow-up. Patients with polyostotic fibrous dysplasia (multiple bones affected) may need closer monitoring and, in some cases, additional treatment. In very rare cases (less than 1%), fibrous dysplasia can develop cancerous changes, although this is uncommon.
Surgery may be recommended in certain situations, such as to prevent a fracture in a weakened bone, treat a broken bone (pathologic fracture) or correct bone deformities or uneven leg lengths.
Because fibrous dysplasia is a rare bone condition that can sometimes look similar to other bone tumors or cause complex bone deformities, evaluation by an orthopaedic oncologist can be helpful. Orthopaedic oncologists have specialized training in diagnosing and treating rare bone tumors and tumor-like conditions, helping ensure an accurate diagnosis and the most appropriate treatment plan.
More Information:
- https://orthoinfo.aaos.org/en/diseases--conditions/fibrous-dysplasia
- https://www.cancer.gov/pediatric-adult-rare-tumor/rare-tumors/rare-bone-tumors/fibrous-dysplasia
- https://www.childrenshospital.org/conditions-treatments/fibrous-dysplasia
- https://www.chop.edu/conditions-diseases/fibrous-dysplasia
This is not intended as a substitute for professional medical advice and does not provide advice on treatments or conditions for individual patients. All health and treatment decisions must be made in consultation with your physician(s), utilizing your specific medical information. Inclusion in this is not a recommendation of any product, treatment, physician or hospital.